---------------------------------------
BY ANISH KOKA
Myopericarditis is a now a well reported complication associated with Sars-Cov-2 (COVID-19) vaccinations. This has been particularly common with the messenger RNA (mRNA) vaccines (BNT162b2 and mrna-1273), with a particular predilection for young males.
Current guidance by the Australian government “technical advisory groups” as well as the Australian Cardiology Society suggest patients who have experienced myocarditis after an mRNA vaccine may consider a non-mRNA vaccine once “symptom free for at least 6 weeks”.
A just published report of 2 cases from Australia that document myopericarditis after use of the non-mRNA Novavax vaccine in patients that had recovered from mRNA vaccine myocarditis suggests this is a very bad idea.
The case reports
Case 1 involves a 26 year old man who developed pericarditis after the Pfizer vaccine. Pericarditis, an inflammation of the sac the heart lives in, developed about 7 days after the Pfizer vaccine. The diagnosis was made based on classic findings of inflammation on an electrocardiogram associated with acute chest pain. The symptoms lasted 3 months, and a total of 6 months after the first episode of pericarditis, he received a booster vaccination with the Novovax (NVX-CoV2373) vaccine. 2-3 days after this he developed the same sharp chest pain and shortness of breath with elevated inflammatory markers (CRP) as well as typical findings of pericarditis seen on ECG. To add insult to injury, he contracted COVID 2 months after the second episode of pericarditis, but had no recurrence of the symptoms of pericarditis.
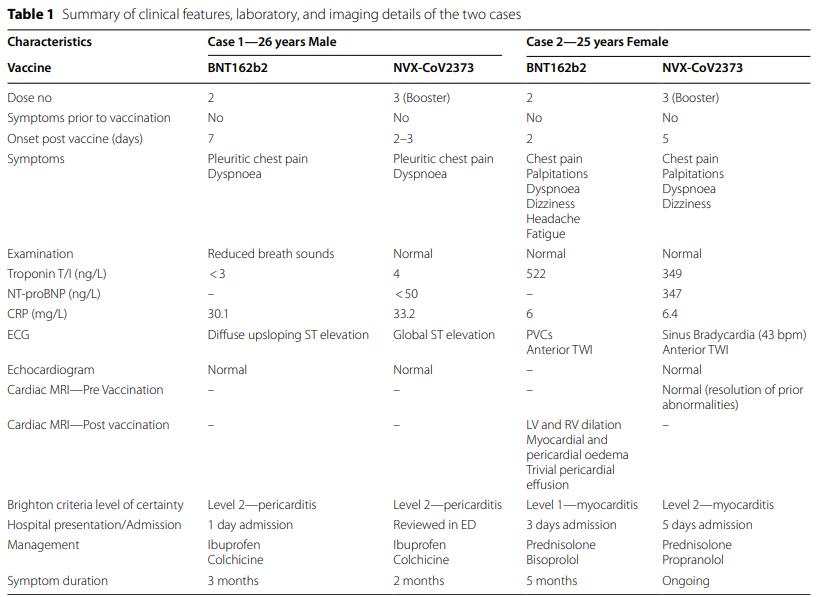
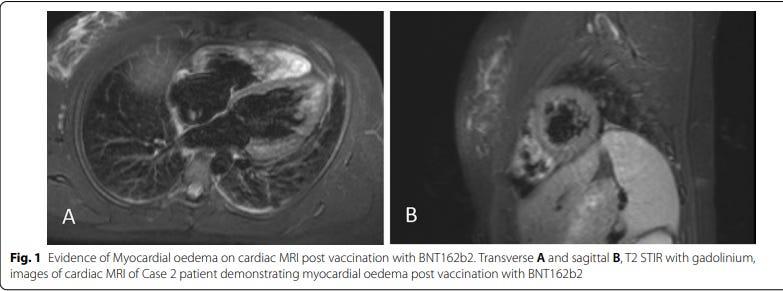
Case 2 involves a 25 year old Australian female who presented with chest pain, shortness of breath and palpitations 2 days after her 2nd dose of Pfizer vaccination. Abnormal cardiac biomarkers suggested damage to the heart muscle confirming myocarditis. The distinction between pericarditis and myocarditis generally hinges on the presence of damage to the cardiac muscle that’s discovered based on blood tests for cardiac biomarkers that suggest ongoing damage/necrosis of heart cells. Case 1 was a case of pericarditis, not myocarditis, because there was no evidence of damage to cardiac cells (cardiac blood test Troponin biomarkers were not elevated).
Myocarditis is generally considered a more serious clinical condition because of the association of damage to the cardiac muscle that is, unfortunately, irreversible. Her course was, as a result, more complicated with persistent symptoms that required recurrent hospital presentations for 5 months. While two-thirds of patients in the pediatric US experience demonstrate a persistent scar on cardiac MRI at 6 month follow-up, a repeat MRI in this case was normal with complete resolution of previously seen abnormalities.
Remarkably, and I suspect in no small part due to the guidance of the Australian technical advisory committee, and the defacto blessing of the Australian cardiac society, she went on to be vaccinated with the Novovax vaccine. 5 days later she once again complained of chest pain, shortness of breath and palpitations. An evaluation revealed another episode of myocarditis. She has had multiple repeat hospital presentations and 2 months later continues to be symptomatic.
There is no clinical history or context provided to help us understand why these two young people needed another COVID19 vaccine booster. It is certainly possible both were considered very high risk for developing a serious COVID infection, but that information is not provided in the published case report. Recall, that the young man in case 1 still went on to contract COVID-19 even after his Novovax booster.
These cases, while unfortunate, do provide some very important insights about the potential mechanism of vaccine associated myocarditis.
Vaccine myocarditis : mechanistic insights
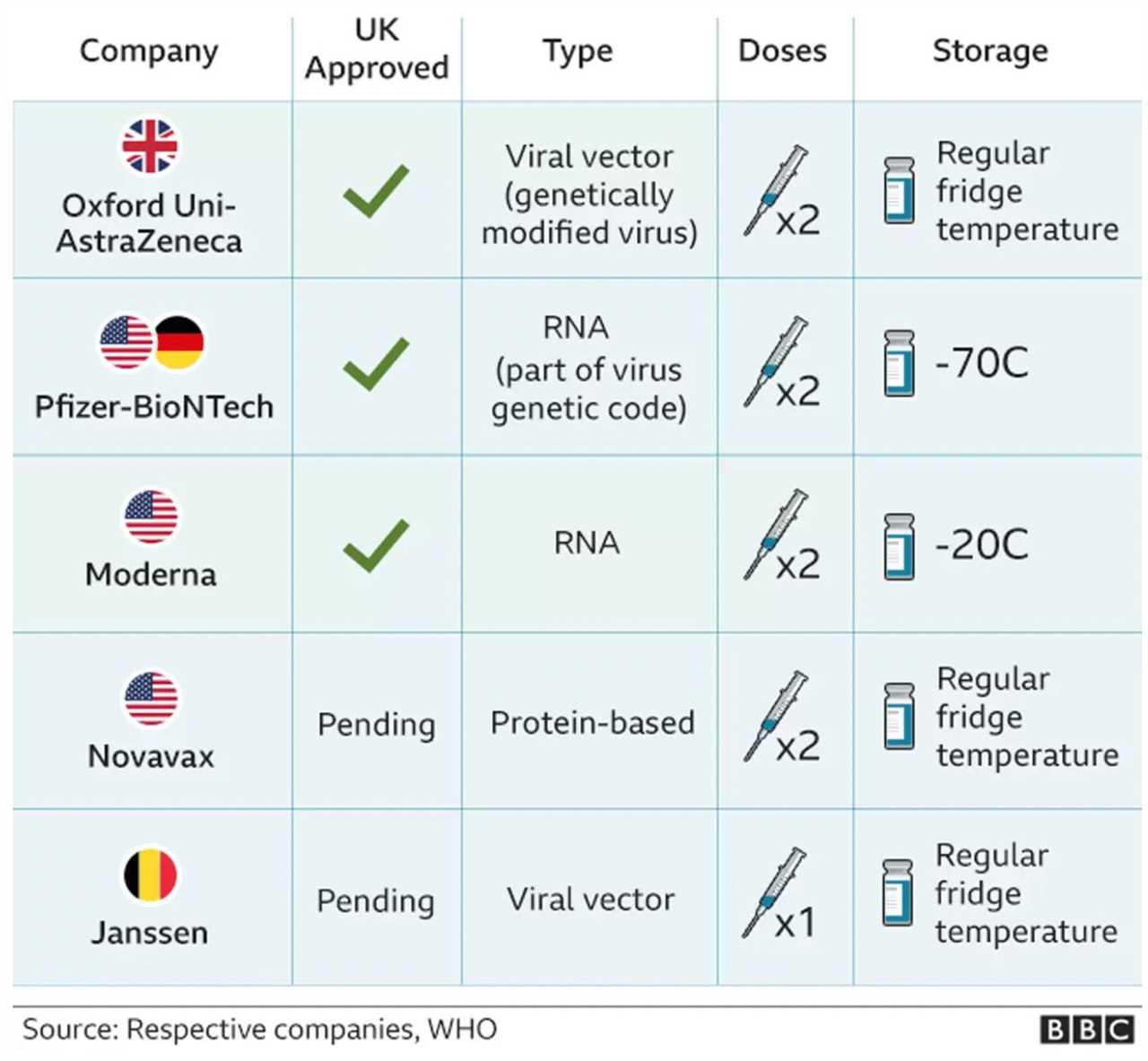
The molecular mimicry theory posits that antibodies the body is induced to produce to the viral S-protein also may recognize parts of the body as foreign and attack itself. But the molecular mimicry hypothesis should result in similar rates of vaccine myocarditis with mrna and non-mRNA vaccines, and this is clearly not the case. Rates of vaccine myocarditis are clearly lower with the more traditional AstraZeneca protein based vaccine.
Hypotheses to try to explain why the mRNA vaccines specifically seem to have more myocarditis focus on the novel nature of using mRNA as a vaccine delivery vehicle.
It is possible that the mRNA strand that is supposed to be locally taken up by muscle cells in the deltoid muscle in the arm, may not be as prone as a protein based system to staying local and instead may be taken up by far flung organs like the heart. Cardiac cells would then transcribe the mRNA message and “present” the S-protein on their cell surface. The inevitable antibody response would result in the body’s immune system attacking cardiac cells that incorporated the S-protein.
Other hypotheses focus on the delivery platform that makes the normally fragile mRNA stable enough to be used as a vaccine : a lipid “sheath” the mRNA is encased in that is referred to as a lipid nanoparticle (LNP). Lipid nanoparticles have a long history of being used as a drug delivery mechanism and the major issue pharmaceutical companies have struggled with using LNPs is immune activation.
As a result, the prior most commonly used drug delivered in a lipid nanoparticle, the cardiac anti-amyloid drug Onpattro, required pre-medication with a high dose of steroids before every 80 minute infusion to make it tolerable for patients.
The arrival of the Novavax vaccine added to the COVID vaccine armamentarium by taking the viral S-protein and enclosing it in a lipid sheath, which is distinct from the widely used Moderna/Pfizer product that encloses RNA in a lipid nanoparticle, and the Oxford-AstraZeneca and Janssen product that puts DNA in a viral vector.
If vaccine myocarditis was primarily a function of mRNA, the protein based Novovax vaccine would hopefully be able to deliver protection from COVID without the risk of myocarditis. Unfortunately, the occurrence of 2 almost identical presentations of myopericarditis with the Novovax and mRNA vaccine suggests otherwise.
The tragedy here is that this wasn’t a surprise. Myocarditis and/or pericarditis were reported by two participants after the Novavax COVID-19 Vaccine, Adjuvanted (0.01%) and no participants after placebo. Events of cardiomyopathy or cardiac failure were reported by eight participants after the Novavax COVID-19 Vaccine, Adjuvanted (0.03%) and one participant after placebo (<0.01%). Per the FDA Emergency Use Authorization, the available information on cardiomyopathy or cardiac failure was insufficient to determine a causal relationship with the vaccine.
Post-approval surveillance brought to light more cardiac activity of the Novovax vaccine. Among a total of 41,546 vaccine recipients aged ≥16 years, six cases of myocarditis or pericarditis were detected; five occurred within 20 days of vaccination. Among these five, four did not have likely alternative etiologies, suggesting a possible causal relationship with vaccine.
In global post-authorization surveillance, among 744,235 doses of Novavax COVID-19 vaccine administered in Australia, Canada, the European Union, New Zealand, and South Korea, 35 reports (representing 36 adverse events) were identified among 20 male and 15 female vaccine recipients with a median age of 34 years (range = 23–62 years).
The 2 case reports from Australia aren’t even the first reports of Novovax myocarditis after mRNA vaccine myocarditis. In July, the CDC reported 29 cases of pericarditis, including five in persons with a history of pericarditis after mRNA COVID-19 vaccine; four myocarditis cases; two myopericarditis cases; and one case of carditis, not otherwise specified. A postmarketing analysis from Australia also identified three cases of myocarditis and 12 cases of pericarditis reported during a period in which 160,000 Novavax COVID-19 vaccine doses were administered.
So even though the US CDC had noted cases of Novovax vaccine related myocarditis in August 2022 in patients with a prior history of mRNA pericarditis, the Australian guidelines fail to list a prior history of mRNA vaccine myocarditis as a contraindication to future COVID19 vaccinations.

If you dig a little bit you will eventually find that the current US CDC guidelines is actually more sane than the Australian guidelines and generally advises prior mRNA vaccine myocarditis cases not receive subsequent doses of any COVID-19 vaccine.
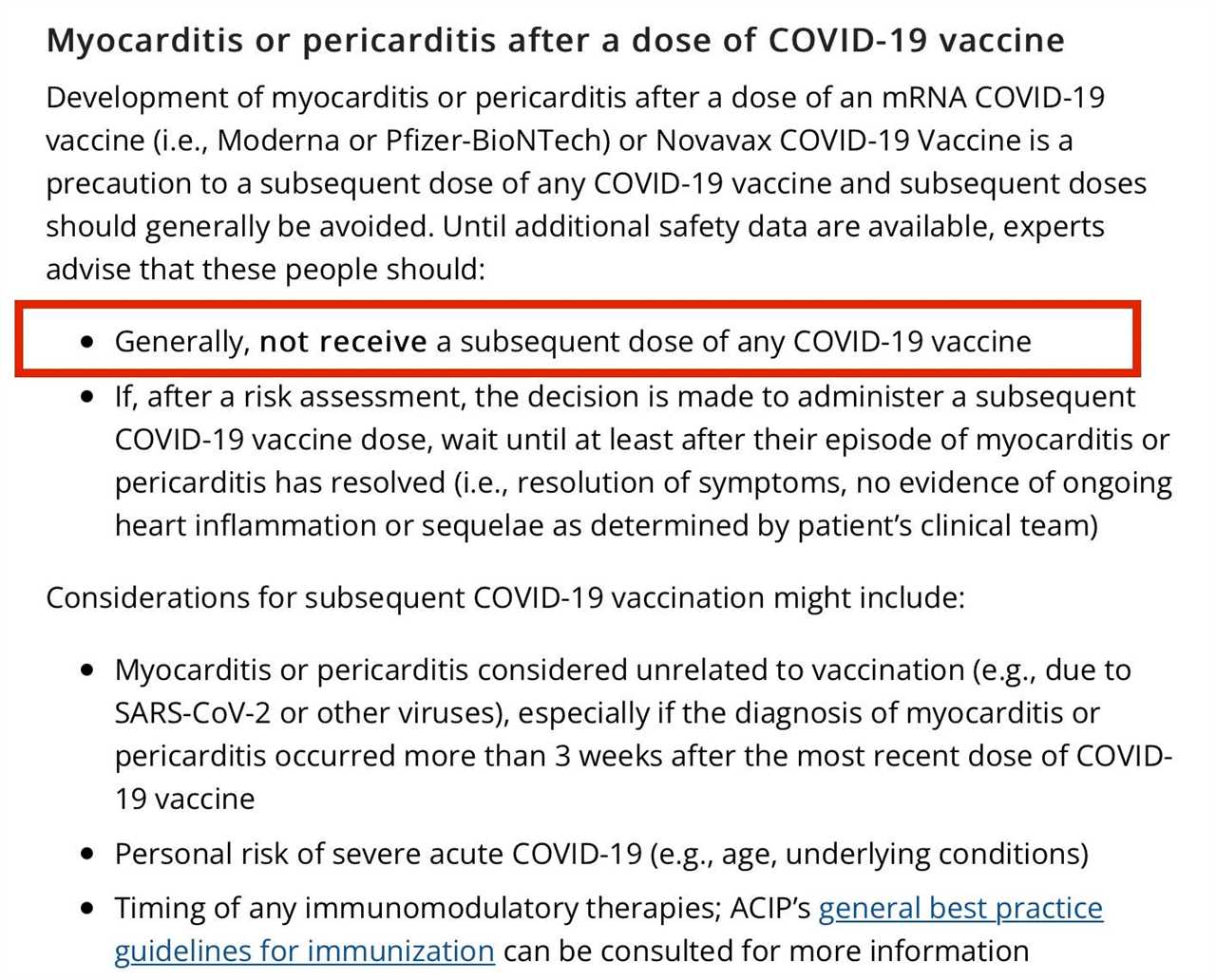
It is a bit confusing as you can see from the CDC summary that recommends COVID-19 vaccination for everyone 6 months of age and older because “the benefits… outweight the risk of myocarditis and pericarditis after receipt of mRNA COVID-19 vaccines”
The just published case-reports should be the nail in the coffin for anyone, anywhere trying to give a COVID-19 vaccine to someone with a prior episode of COVID-19 vaccine myocarditis.
Despite the fact vaccine myocarditis has been associated with the Novovax vaccine since the trials that lead to its approval in the US, vaccine advisory panels and medical societies seemingly stuck their heads firmly in the sand. Those in charge of vaccine policy were so averse to recommending against vaccine administration to anyone, that they couldn’t even explicitly warn those with a prior episode of COVID vaccine myocarditis against receiving future COVID vaccines.
The Novovax myocarditis cases that occurred after the US CDC summer analysis were clearly preventable adverse events. It is very hard to understand, even without this data, how physicians or medical societies sanctioned administration of a COVID vaccine to those who had already had COVID vaccine myocarditis.
Interestingly, the Novovax social media team has clearly picked up on the prevailing mRNA vaccine hesitancy to try to generate demand for their product at a time there is very little demand for any COVID vaccines.
The story is a nice distillation of what lies at the heart of the outsize influence random dudes on twitter have developed relative to White House COVID czars. If the real leaders of medicine can’t critically analyze the data to explicitly recommend against those with prior COVID vaccine myocarditis receiving future COVID vaccines, what else are they getting wrong?
Our public health officials are just not very good. The scorn much of the public feels for the institutions and the credentialed class that purport to have the public’s best interest at heart is well earned. Hopefully Santa has stuffed their stockings with common sense for the New Year.
I’m not holding my breath.
Anish Koka is a cardiologist. Follow him on Twitter @anish_koka.
I have to make the obligatory post-script here that I oversaw the administration of hundreds of mrna vaccines starting in March of 2021 in my cardiology clinic. The vaccine efficacy data for the original data was from thousands of patients and I certainly felt given the devastation wreaked on many of my patients in 2020 that the vaccines were the best chance of avoiding morbidity and mortality. The process to get the vaccines from the city department of health was a somewhat arduous 3 month process, and once the vaccines were on hand, there were daily reporting requirements that I dutifully performed for the many months we were administering vaccines. To accommodate the rush of patients, employees, volunteers, and conscripted children worked multiple weekends to administer the vaccines. So I’m especially disgusted by medical colleagues who label any concerns registered about vaccine adverse events as “anti-vaxx”. Registering concern over a vaccine adverse event does not make doctors or patients “anti-vaxx”. It makes them pro-vaxx!
-----------------------------------------
By: Ryan Bose-Roy
Title: Cardiology update: Should mRNA vaccine myocarditis be a contraindication to future COVID-19 vaccinations ?
Sourced From: thehealthcareblog.com/blog/2023/01/26/cardiology-update-should-mrna-vaccine-myocarditis-be-a-contraindication-to-future-covid-19-vaccinations/
Published Date: Thu, 26 Jan 2023 10:16:00 +0000
Read More
Did you miss our previous article...
https://prohealthsciences.com/general-health-and-wellness/ultrasound-is-ultracool
